Goal
Achieve complete regression of metastatic cancers, especially breast cancer, by targeting patient-specific tumor mutations.
Problem
Metastatic breast cancer unresponsive to standard chemotherapy, hormonal therapy, and other treatments.
Concept Summary
A personalized immunotherapy that sequences a patient's tumor to identify somatic mutations, isolates tumor-infiltrating lymphocytes (TILs) that recognize mutant proteins, expands those TILs ex vivo, and reinfuses them together with checkpoint-inhibitor antibodies and IL-2 to induce a durable anti-tumor immune response.
Principles
- Adoptive cell transfer
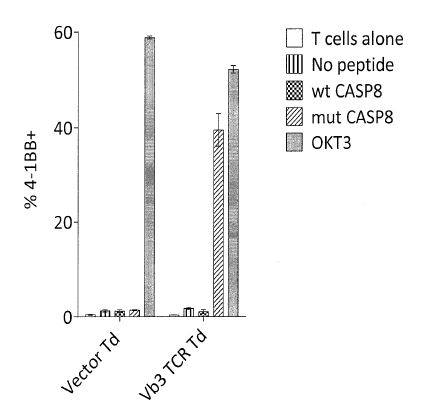
- Mutation-specific T-cell targeting
- Checkpoint inhibition
- Cytokine support (IL-2)
Scientific Domains
Materials
- Peripheral blood mononuclear cells (PBMCs)
- Tumor-infiltrating lymphocytes (TILs)
- Cytokine IL-2
- Checkpoint inhibitor pembrolizumab (anti-PD-1 antibody)
Mechanisms of Action
- TILs recognize neo-antigens presented on MHC molecules
- PD-1/TIM-3 enrichment selects tumor-reactive T cells
- Checkpoint blockade prevents T-cell exhaustion
- IL-2 promotes T-cell proliferation after infusion
Applications
- Treatment of metastatic breast cancer
- Personalized therapy for other mutation-bearing epithelial cancers
Claimed Performance
Complete durable regression of metastatic breast cancer lasting >22 months after infusion of ~90 billion TILs; similar responses reported in other epithelial cancers.
Experimental Evidence
Case report of a single metastatic breast-cancer patient (Nature Medicine, 2018) and ongoing Phase 2 clinical trial (NCT01174121) showing tumor shrinkage in multiple patients.
Replication Status
Only a single-patient case report confirmed; larger Phase 2 trial ongoing but results not yet published.
Limitations
- Requires individualized tumor sequencing
- Complex, labor-intensive cell manufacturing
- Efficacy limited to patients whose tumors harbor immunogenic mutations
- Current evidence limited to small case series